Disruptive Innovation in the halls of UNE

Call it fate, call it coincidence, call it serendipity. Call it whatever you want, but when UNE President James Herbert refers to the events leading to a major discovery about the Zika virus in UNE labs, he calls it “the hallway story.”
We are all familiar with another, tangentially related – though far more well-known — tale of how Scottish researcher Sir Alexander Fleming discovered penicillin in 1928. After returning to his lab from a two-week vacation, before which he had failed to clean his work space, he found that contaminated samples of the staphylococci, which he had been culturing, had been killed off by the growth of a blue-green mold. (Fleming had a reputation for being a bit of a slob.)
Maybe it’s not so uncommon for scientific discoveries to unfold with a certain degree of happenstance in the mix. But the type of novel approach to research and scholarship that President Herbert champions, exemplified by the Zika discovery at UNE, doesn’t rely quite so much on pure accident as the discovery of penicillin. (So sorry, UNE scientists, the president isn’t doling out free passes to chuck your petri dishes in the sink and call it a day.) The breakthrough moments that Herbert admires, rather, are the ones that Associate Professor of Biomedical Sciences (and focal character in the hallway story) Meghan May calls examples of “disruptive innovation.”
May’s findings about the Zika virus, as this tale will describe, were the result of a series of coincidences, true. But unlike mold growing in a dirty lab, these events didn’t happen as the result of human inaction. Rather, it was the culmination of human curiosity, camaraderie, and cooperation that sparked a significant — and potentially life-saving — discovery.
In was back in March of 2016 when May, a microbiologist, unexpectedly received an invitation to attend the Zika Global Health Symposium. At that point in time, microbiologists had had limited involvement with Zika. Some had looked at Zika genome sequencing, and some had figured out how to grow the virus in the lab, but it was the clinicians who were on the front lines, battling a disease that had reached epidemic proportions. They were up against an infectious organism that had transformed from a sporadic and somewhat mild virus in Africa and Asia (documented as far back as the early 1950s), which produced fever and rash, to an illness spreading like wildfire in South America in 2015, sometimes accompanied by encephalitis (or brain swelling) and horrific birth defects, namely microcephaly (abnormal smallness of the brain), in babies born to infected mothers.
“This epidemic was starting to have a ‘the-sky-falling’ feel to it. It was getting pretty terrifying,” says May. “And physicians didn’t really have much of anything reassuring to tell people. There was no test; there was no vaccine; there was no medication.”
May, having recently traveled to two other nonrelated conferences, had no intention of attending the Zika Symposium. “Honestly, I thought I received the invitation by mistake,” she admits. But when she noticed it was to be held in nearby Boston, she figured, “Why not?”
This epidemic was starting to have a ‘the-sky-falling’ feel to it. It was getting pretty terrifying. And physicians didn’t really have much of anything reassuring to tell people. There was no test; there was no vaccine; there was no medication.”
-- Associate Professor Meghan May
Of the 50 attendees, May was one of about a dozen scientists present. There were also policymakers in attendance, but most participants were clinicians: doctors and nurses — as well as social workers, who offered a unique perspective on the familial and social service strains that the birth of Zika-infected babies were having in South America.
“As scientists, we were learning nuanced information that we usually don’t learn from clinicians because usually scientists and clinicians don’t collaborate,” May shares. “It’s like we’re New York, and they’re New Jersey. Yeah, there’s a bridge, but it’s got traffic, and it’s got a toll booth; so why drive across a bridge to go to a Chipotle in New Jersey when there’s one over here?” she says with a chuckle at her own metaphor.
May credits the urgency of the global Zika crisis with changing the usual dynamics. The experience of having scientists, clinicians, and policymakers all working together on a time-sensitive problem of such magnitude effectively broke down the old barriers. “It was like we were our own island with one taco stand,” she says.
May walked away from the symposium with not only a deeper understanding of the social ramifications of the disease but a few nuggets of wisdom from doctors. They noted that unlike sufferers of the earlier generation of Zika, who had rashes but no itch, the “new” Zika victims were plagued by an uncomfortable pruritus. And they pointed out that while viral-induced encephalitis usually causes delusions and ataxia (problems with physical coordination), patients with Zika-induced encephalitis were clumsy but not confused. May was grateful that the physicians hadn’t ignored the presentation of anomalies that didn’t fit with the sets of symptoms they previously knew about. “I left the symposium thinking, ‘That was clever of them to pick up on those things,’” she remembers.
So, even more deeply impacted than before by her expanded view of Zika, energized by the opening up of communication channels with clinicians, and maybe even feeling a renewed respect for their diligence, May came back to UNE and started to look at Zika through her own lens of expertise. She began studying the genome sequencing of the older African strains of Zika compared to those of the newer South American strains, zoning in on parts of the DNA where the two types significantly differed from one another.
“What we found is that the new strains of Zika have actually changed the way that they attach to cells. And because they have a different way of attaching to cells, they are able to attach to different types of cells — different from those that the African strains of Zika were able to attach to,” May explains. “African Zika, for example, couldn’t attach to brain cells, but the South American virus can, and that’s why we see encephalitis with the newer version of the virus.”
According to May, the same mutations that allowed the virus to attach to other kinds of cells, unfortunately, also gave it the ability to cross the placenta, thereby explaining the birth defects resulting from South American strains.
And here is where the hallowed halls of UNE factor into “the hallway story.”
Derek Molliver is an associate professor of neuroscience at UNE. And like many other faculty members in the sciences at the University, he happens to be friendly with May.
“I was just chatting with Derek one day in Stella Maris Hall, and I mentioned the work I was doing on Zika. I knew that his lab specializes in extracting dorsal root ganglion neurons. I didn’t know exactly what these were, but I knew that they come from the brain, and I was interested in testing my suspicions that South American Zika binds to brain cells. So, I said, ‘Hey, do you think I could have some of those cells you work on so I can see if the virus will stick to them?’ And he said, ‘Sure.’”
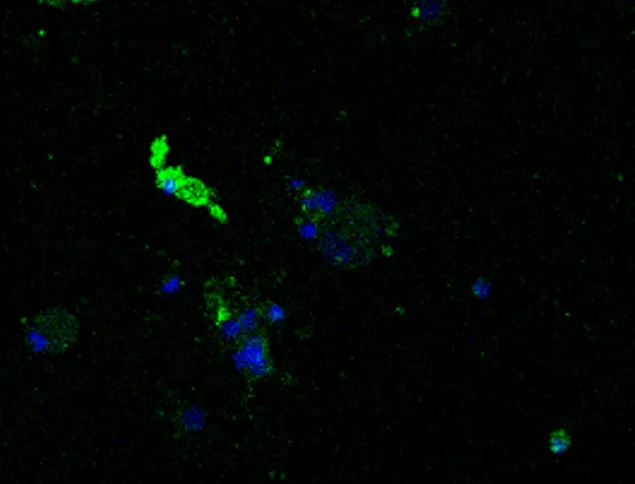
So, Molliver’s technician grew some cells that were tagged with a blue fluorescent dye, and May’s technician grew batches of old Zika and new Zika, both tagged with green. May and Molliver put some of each batch together with the brain cells and watched to see what would happen.
The new Zika cells, to May’s delight, were binding to the brain cells. “‘I was like, Wow! My green virus is attaching to your blue brain cells!’” recalls May. “At that point, I could have just said, ‘Great. They bind. That confirms my findings with the genome sequencing. We’re done here,’ but that’s not where it ended,” she says. “Derek said, ‘You know, if this were to happen in a person, there would be some very specific symptoms. And I said, ‘Well, the most commons symptoms of Zika are fever and rash,’ and Derek asked, “What is the rash like?’ and I said, “I’ve heard it’s itchy.’”
May says that Molliver gasped. It was then that he told her that the dorsal root ganglion neurons he gave her are the specific type of cells responsible for the sensation of itchiness.
“To me, it was important that the virus had bound to these brain cells, but the exact type of brain cells wasn’t particularly meaningful to me. To a neuroscientist, though, it meant something very specific, which ended up being extremely significant,” says May.
May now had evidence to support the idea, indicated by the genome sequencing, that the new Zika was capable of binding to brain cells, and, furthermore, she had verification that the virus binds to a specific type of brain cell that would correlate with actual Zika symptoms.
“If the clinicians at the symposium hadn’t happened to mention the itchiness factor, and if I hadn’t happened to be friendly with a neuroscientist colleague who works with dorsal root ganglion neurons, the affirmation of my observations of the genome sequencing would never have happened,” says May with a bit of wonder. “It was a neat series of the right people having the right conversations.”
Interestingly, the hallway conversation with Molliver was not the only coincidental collegial interaction that confirmed May’s findings. One day, not long after the experiment, May was having lunch with Associate Professor Tamara King, a physiologist, and May was sharing some of the successes — and limitations — of her Zika research.
“I was telling Tamara about what Derek and I had found, but I was saying, ‘You know, causing Zika cells to bind to brain cells outside of the body is one thing; finding out if they would actually bind inside the body would be really cool,” reports May. King, whose expertise is in the analysis of pain, routinely gives intravenous injections to mice in order to conduct her research. She suggested to May that she inject a mouse with Zika to see if the same binding action would occur.
May went to UNE’s Imaging Core to conduct the experiment. Again, she tagged a batch of “old” Zika cells and “new” Zika cells with a fluorescent green dye. Both batches were injected into two different sets of mice, respectively, and dissection followed. May and King checked the mice’s spleens, and, as would be expected, both types of Zika were present in the respective mice. Then, they checked the brain and spinal cord tissue. In the mice who received the old Zika, the tissue was unaffected. The tissue of the mice injected with new Zika, however, had turned green. “I was so excited to see that Zika binds to these tissues in an actual animal and not just when artificially put together,” said May.
King, who happened to be in the Imaging Core helping a student, walked by May’s microscope and took a peek. She asked May if she knew what she was looking at. “I said, ‘Yeah, of course I know what I’m looking at; it’s a spinal cord,’” May recalls with a laugh. With King’s curiosity peeked by what she saw, she asked May about the symptoms of Zika. When May mentioned that Zika sufferers present with clumsiness but normal cognitive function, King gasped.
King explained to May that what the microscope revealed was far more interesting than just Zika cells binding to the spinal cord. The area of the spinal cord that was shining green with Zika cells was a very specific area of the spinal cord: the ventral horn.
The ventral horn of the spinal cord is responsible for motor function, while the dorsal side is responsible for cognitive function. The fact that the encephalitis that Zika patients develop renders them uncoordinated but not cognitively impaired all made sense. It was one more piece of proof that the old Zika had adapted its DNA to bind to cells to which its predecessor could not bind – cells that, when infected, would logically produce the very symptoms that Zika patients experience.
“Again, if I hadn’t been at the symposium where doctors were sharing clinical information with scientists, I would have had no idea that Zika-induced encephalitis was different from any other encephalitis, which normally produces both deliriousness and ataxia,” May says. “And if I hadn’t been lunch buddies with Tamara, who offered me the opportunity to see the cellular response in an animal, rather than in a dish, this never would have been confirmed; it just would have remained a clinical observation — not a scientific one.”
May is quick to acknowledge that the discovery involved a group effort. “This wasn’t one person’s ‘aha moment,’” she states. “This was three people’s ‘aha moment.’ And if we hadn’t had these random conversations, these serendipitous exchanges, then these findings never would have been made.”
This wasn’t one person’s ‘aha moment.’ This was three people’s ‘aha moment.’ And if we hadn’t had these random conversations, these serendipitous exchanges, then these findings never would have been made.”
-- Associate Professor Meghan May
May views herself as the common denominator in three dialogues that unfolded with little rhyme or reason. Even her attendance at the symposium, which had initially sparked her interest in Zika, felt like an opportunity that fell out of the sky. “To this day, I have no idea why I was invited,” she puzzles.
“But If there hadn’t been clinicians there who were willing to tell me, a microbiologist, about the odd symptoms of Zika patients, and you didn’t have me, the microbiologist, talking to a neuroscientist friend who said the Zika virus is attaching to brain cells that cause itchiness, and you didn’t have me, the microbiologist, talking to a physiologist lunch pal who said, the attachment is taking place in the ventral horn of the spinal cord and not the dorsal horn, then we wouldn’t be where we are right now,” May exclaims.
So aside from being a compelling narrative about groundbreaking research coming out of UNE and a tale that takes a lot of unexpected turns (because, of course, everyone loves a good plot twist), why is Herbert so fond of the hallway story?
He answers this with a continuation of May’s metaphor by declaring that “it’s not only necessary to build a bridge between New York and New Jersey, but there need to be accessible roads between Brooklyn and Queens too.”
He elaborates: “Clinicians need to talk to scientists, and different kinds of scientists have to talk to one another, and I think the story demonstrates the sort of spontaneous innovation that happens every day at UNE. Now, it may not lead to groundbreaking research every day, but interprofessional and intraprofessional dialogue is happening, and this story is a testament to that. But the story also makes us realize that we don’t have to just rely on organic hallway chatter for these synergistic opportunities. If something as amazing and as potentially useful as these Zika findings can be born of happenstance, think of what we could accomplish if we purposely made concerted efforts to join forces across specialties. When we put disparate expertises together, great things can come from it.”
If something as amazing and as potentially useful as these Zika findings can be born of happenstance, think of what we could accomplish if we purposely made concerted efforts to join forces across specialties. When we put disparate expertises together, great things can come from it.”
--President James Herbert
May agrees that it shouldn’t take an international crisis like Zika for people to work together. “I’m a big believer in fate, and I accept nudges from the universe,” she shares, “but we can also do things purposely and proactively to share what we know, to seek out other opinions, to learn from others’ knowledge — because you don’t know what it may spark.”
So if there is a moral to “the hallway story,” what would it be? That New Jersey Chipotles have different menus from the ones in New York? To always have a buddy look through your microscope? That it’s OK to live in Brooklyn as long as you still visit Manhattan?
Or maybe it’s that at UNE, no detentions will be given for talking in the hallway.
(Though you might get one for not cleaning up your lab.)